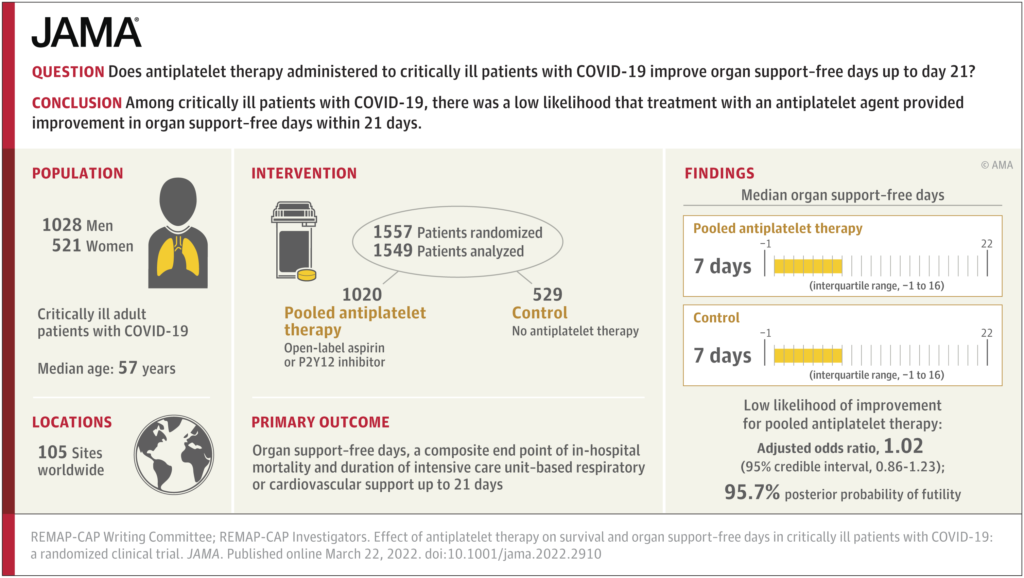
Importance The efficacy of antiplatelet therapy in critically ill patients with COVID-19 is uncertain.
Objective To determine whether antiplatelet therapy improves outcomes for critically ill adults with COVID-19.
Results
The aspirin and P2Y12 inhibitor groups met the predefined criteria for equivalence at an adaptive analysis and were statistically pooled for further analysis. Enrollment was discontinued after the prespecified criterion for futility was met for the pooled antiplatelet group compared with control. Among the 1557 critically ill patients randomized, 8 patients withdrew consent and 1549 completed the trial (median age, 57 years; 521 [33.6%] female). The median for organ support–free days was 7 (IQR, −1 to 16) in both the antiplatelet and control groups (median-adjusted OR, 1.02 [95% credible interval {CrI}, 0.86-1.23]; 95.7% posterior probability of futility). The proportions of patients surviving to hospital discharge were 71.5% (723/1011) and 67.9% (354/521) in the antiplatelet and control groups, respectively (median-adjusted OR, 1.27 [95% CrI, 0.99-1.62]; adjusted absolute difference, 5% [95% CrI, −0.2% to 9.5%]; 97% posterior probability of efficacy). Among survivors, the median for organ support–free days was 14 in both groups. Major bleeding occurred in 2.1% and 0.4% of patients in the antiplatelet and control groups (adjusted OR, 2.97 [95% CrI, 1.23-8.28]; adjusted absolute risk increase, 0.8% [95% CrI, 0.1%-2.7%]; 99.4% probability of harm).